Data Rich, Capture Poor: How Automation-Assisted IVF Multiplies Data Density
Conceivable Life Sciences | “The Case For Automation” Series | No. 2

A patient's cycle produces unexpectedly few blastocysts. The clinical team needs to understand why. Which would be more useful to have in front of them?
A. The embryologist's recollection of the cycle, the standard morphology grades, and handwritten notes on the lab worksheet.
B. A complete, timestamped record of every procedural step, environmental condition, and image captured across the cycle — structured the same way as every other cycle the lab has run.
Every IVF cycle generates thousands of biological signals: temperature shifts, timing intervals, environmental fluctuations, procedural decisions, each one potentially relevant to what happens to the embryo. Most of it is carried in an embryologist's hands and memory, and when the cycle ends, most of it disappears.
The IVF lab generates far more biologically meaningful information than it captures. Manual workflows record what a person notices, at preset intervals: a morphology score, an environmental log, a procedural note entered at the end of a session. The result is a record of endpoints, not process. The fluctuations, the intervals, the decisions made between observations go largely undocumented. Automation assistance is built on a different premise: that capturing the full record of a cycle should be a function of how the lab runs, built into the workflow rather than added on top of it.
The Problem : A Capture Gap, Not A Data Gap
The IVF laboratory has, over the last two decades, accumulated impressive point solutions for capturing what happens to gametes and embryos. Time-lapse incubators generate continuous imaging and environmental records for the embryos cultured inside them. Electronic witnessing systems log identity-critical handling events. Quality management systems track media lots, incubator alarms, and equipment calibration. Individually, each addresses a real gap. Collectively, they do not yet constitute a process record. The IVF laboratory is an information-rich environment, it generates thousands of biological signals per cycle. It needs the infrastructure to capture, structure, and retain them. A typical cycle generates a small set of recorded observations such as fertilization rate, cleavage stage, blastocyst grade, transfer outcome. Between those checkpoints, the lab is effectively running blind. Data points such as temperature fluctuations during dish handling, timing intervals between procedural steps, and subtle differences in technique between operators are not captured systematically. As the field moves toward greater transparency and auditability, a complete process record covering everything that happened to a patient's biological material, becomes an expectation rather than an exception. In a manual lab, that record is incomplete, and often inaccessible.
The consequences play out across three distinct moments. During a cycle, the clinical team cannot see what is actually happening between observations: the temperature that shifted during a handling step, the interval that ran longer than protocol, the technique that varied between operators. After a cycle, if outcomes are poor, there is no process record to investigate. The team cannot necessarily distinguish a biological failure from a process failure, or trace cause with credible evidence. And across cycles, even the observations that are recorded are not standardised — morphology grading is subjective and timing conventions vary between operators, making records difficult to aggregate meaningfully. Without consistent, structured data accumulating over time, the foundation needed for meaningful research or predictive modelling never forms. The Vienna Consensus called for systematic, transparent, and consistent data collection and KPI tracking across IVF laboratories. The headline KPIs are achievable in a well-run manual lab, but the process-level data layer that would let the field move from KPI reporting to mechanistic understanding remains out of reach.
Conceivable's Approach: The C:NEXUS Platform
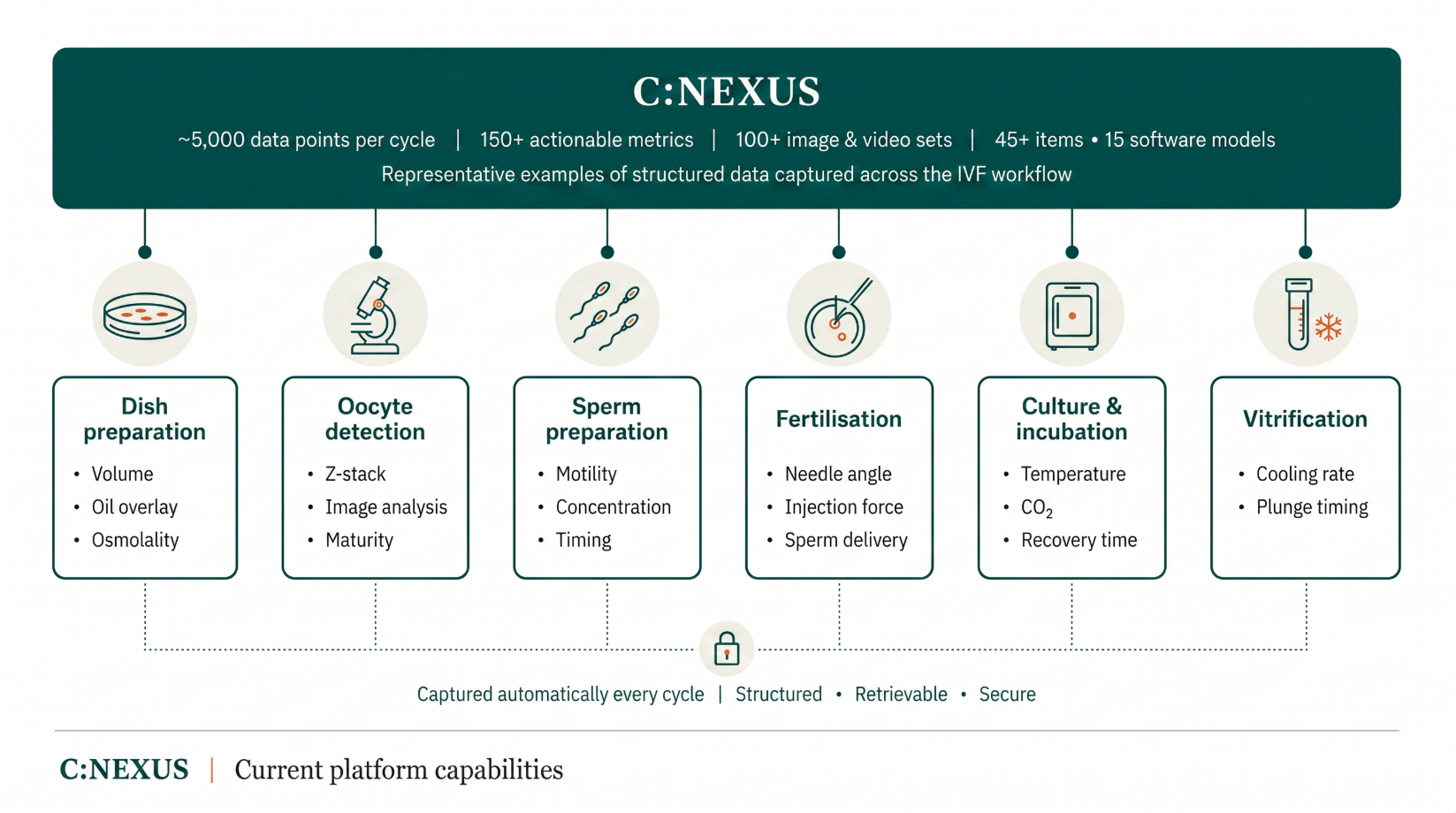
Conceivable's response to that gap is architectural rather than incremental. AURA is a suite of robotic instruments, each designed to provide automation assistance for one step of the IVF workflow; dispensing, imaging, labelling, sperm and egg preparation, fertilisation, culture, and vitrification. C:NEXUS is the software layer that connects them. A central order manager tracks every specimen, routes it through the correct sequence, and logs every action taken at every step, on every instrument, across the full workflow, including the bench-side handling steps that fall outside the incubator and have historically gone unrecorded.
ESIG and Alpha Scientists in Reproductive Medicine 2017. The Vienna consensus: report of an expert meeting on the development of ART laboratory performance indicators. RBMO, 35(5), 494-510.
The resulting difference in data density is substantial: a C:NEXUS-managed cycle generates on the order of 5,000 data points, rising to 8,500+ as full station integration completes, and captures structured outputs from sixteen computational models running across the workflow. This produces a structured record covering the procedural steps, environmental conditions, timing intervals, and imaging that a manual workflow captures only in fragments. The Electronic Laboratory Notebook assembles this into a case record as the cycle runs and timestamps the compliance steps alongside it. The record becomes a product of the workflow itself, the only configuration that guarantees documentation survives time pressure. The Vienna Consensus described what systematic laboratory data should look like; this is what it looks like when the workflow generates it natively.
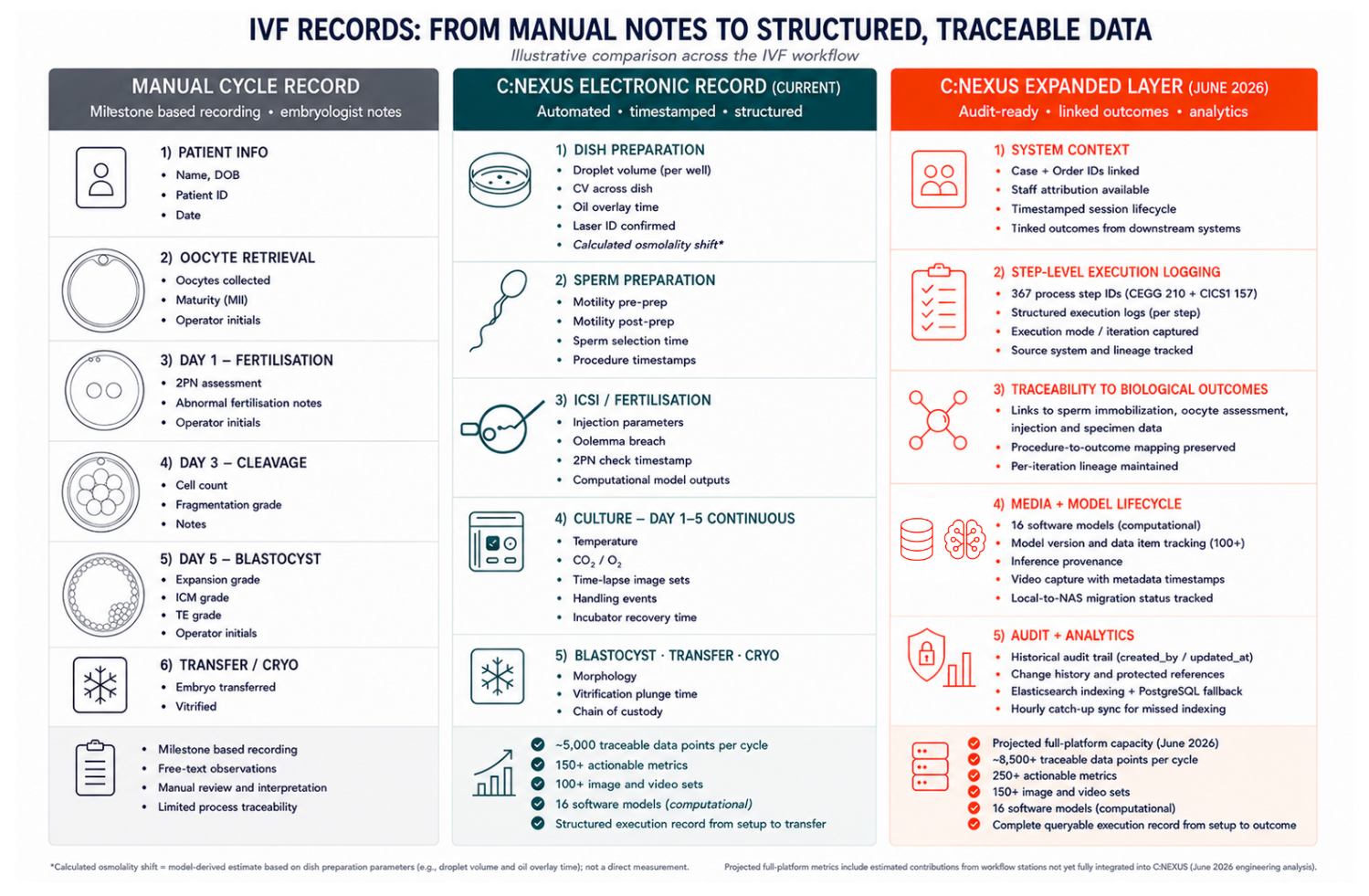
C:NEXUS data capture across the IVF workflow: a representative cycle record compared to manual documentation. Source: Conceivable Life Sciences platform data, June 2026.
The Implication
For the clinical team, the immediate change is diagnostic: a comprehensive process record to interrogate, one where every procedural step is fully traceable and every clinical decision is systematically documented. The implication extends well beyond individual cycle review. IVF research has long been constrained by the same capture limitations that affect clinical practice; studies are underpowered, datasets are heterogeneous, and technical variability between operators and sites confounds any attempt to isolate biological signal from procedural noise. Standardised, continuously captured data across AURA laboratories changes this fundamentally. Multi-center studies become feasible with genuine experimental control. KPIs become comparable across sites. The field gains the consistent, structured datasets it has always needed to answer foundational questions about embryo development, culture conditions, and implantation, rigorously, at scale.
Chavez-Badiola et al. 2025. The Potential of the Automated IVF Lab. Fertility & Sterility, https://www.fertstert.org/news-do/potential-automated-ivf-lab
And looking further forward: the dataset being built todayis the foundation for what becomes possible tomorrow. Predictive models require volume, consistency, and structure. The IVF laboratory that captures everything now is the one best positioned to personalise treatment, anticipate outcomes, and improve results as the science matures. Data density is both an operational advantage and a strategic one that it compounds over time.
The Answer to the Quiz:
A patient's cycle produces unexpectedly few blastocysts. The clinical team needs to understand why. Which would be more useful to have in front of them?
A. The embryologist's recollection of the cycle, the standard morphology grades, and handwritten notes on the lab worksheet.
B. A complete, timestamped record of every procedural step, environmental condition, and image captured across the cycle. Structured the same way as every other cycle the lab has run.
The answer is B. It's the obvious choice, which is why it's worth asking what it would take to actually have it. Most IVF laboratories today operate closer to A than they would like. Time-lapse, electronic witnessing systems, and quality management software have improved what gets captured, but these are not necessarily universally available and records remain fragmented across systems. The handling, the timing, the technique, are still largely held in operator memory rather than in a durable record. The consequence is a field that can report its KPIs but cannot easily interrogate them.
Conceivable's C:NEXUS platform produces option B as a product of how the workflow runs, not as a parallel document. The point is not the volume of data, though the volume is substantial. The point is that it creates the structural conditions for systematic, transparent, consistent data, accumulating in a form that supports both clinical decisions today and the research that will improve them tomorrow.